
The population of the Netherlands is 17,084,467. In 2018 there were 119,923 new cancer cases; 63,910 male and 56,013 female and 47,286 deaths. The top three for men are prostate (19.9%), colorectum (13.3%) and lung (10.2%). For women it was breast (28.9%), colorectum (11.4%), and corpus uteri (3.7%). There are 393,271 people currently living with cancer in the Netherlands.
A higher percentage of the Dutch population die of cancer than in any other EU state apart from Slovenia, according to new research by the European statistics agency Eurostat. In 2015, 1.3 million people died from cancer in the European Union, which equated to more than one quarter of the total number of deaths. However, the share of the total number of deaths which were due to cancer in 2015 exceeded 30 % in the Netherlands and Slovenia. Denmark and Ireland were third and fourth in the ranking.
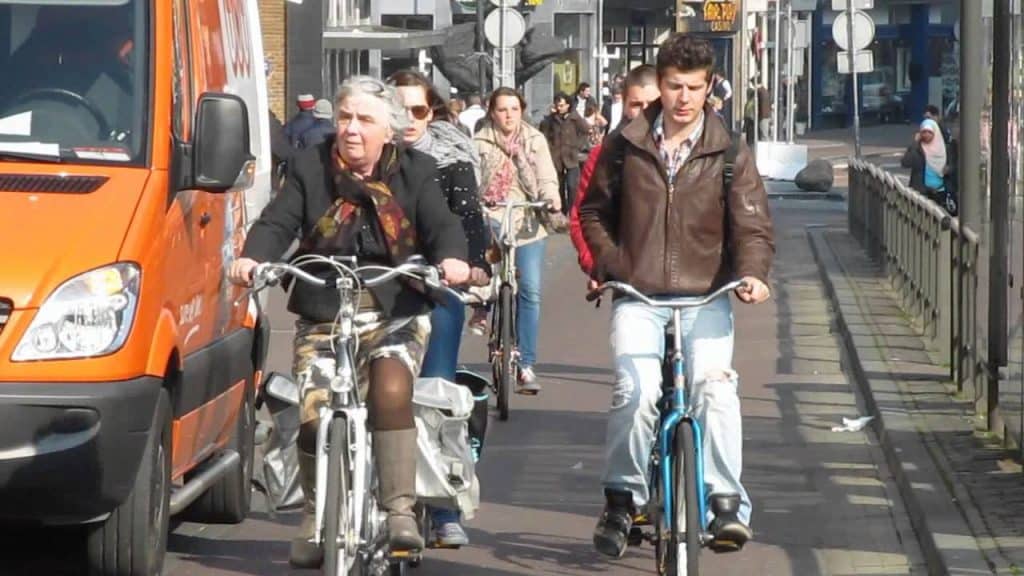
Lung, colon and breast cancer are the most common cancers among women in the Netherlands. Smoking is a huge contributor; many Dutch women have been smoking for decades. In addition, Dutch women have children at a relatively late age, which is also a risk factor in developing breast cancer.
An estimated four in ten premature deaths can be attributed to smoking in the Netherlands. According to a 2017 study by Reep-van den Bergh CMM1, Harteloh PPM, Croes EA, the hazard ratio for premature death was 3.8 (95% CI: 3.2-4.5) for heavy smokers, 2.6 (95% CI: 2.2-3.0) for moderate smokers and 1.7 (95% CI: 1.3-2.3) for light smokers. Lifelong heavy smokers had a chance of 23% of dying before the age of 65. For moderate and light smokers and for non-smokers, the chance was respectively 16, 11 and 7%. For half of all people who died relatively young, cancer was the underlying cause of death. This was mainly lung cancer for smokers. Heavy smokers are estimated to have lost 13 years of life, moderate smokers 9 and light smokers 5. Smoking cessation at any age still benefited health. Ex-smokers who had quit before an approximate age of 35 had the same life expectancy as lifelong non-smokers.
In a study by have shown that the risk of being diagnosed with breast cancer, invasive only as well as invasive and DCIS, in the Netherlands has increased since 1990. The frequently cited breast cancer risk of 1 in 8 women no longer holds, with now 1 in 6.6 women (invasive only: 1 in 7.4 women) receiving a breast cancer diagnosis during their lifetime. Most women are still diagnosed after the age of 50, with a peak between 60 and 70 years. The risk of breast cancer death, on the other hand, has significantly decreased. In the Netherlands, based on 2010 breast cancer mortality rates, 1 in 27 women will die from breast cancer during their lifetime (compared with 1 in 24 in 2000).
Through proper education cancer can be prevented, life expectancy can be increased, and quality of life both during and after treatment can be improved exponentially. The Cancer Exercise Training Institute (CETI), a United States-based organization, has trained over 10,000 health and fitness professionals to become Cancer Exercise Specialists since 2004. CETI and it’s regional affiliates are bringing the Cancer Exercise Specialist Advanced Qualification training to New Zealand and Australia in 2019.
Through the comprehensive training health and fitness professionals seeking to attain a higher level of mastery and work with cancer patients during and after cancer surgery and treatment and into survivorship. Participants will expand their skills as a CES and gain a complete understanding of the entire cancer process from diagnosis and treatment to reconstruction and survivorship. The unique and individualized programming will help to improve the patient’s ability to cope with the mental and physical stress following cancer diagnosis and treatment. The comprehensive programming covers 26 types of cancer, as well as pediatrics, with special emphasis on breast cancer and breast reconstruction.
“The Cancer Exercise Specialist is to CANCER what Cardiac Rehab. is to the HEART PATIENT.” – Andrea Leonard
Regular continuing education is required to maintain the high-standard of expertise required to work with this population.
The benefits of exercise during treatment include:
- Increased energy
- Improved treatment tolerance
- Decrease in pain
- Decrease in depression
- Better sleep
- Improved self-esteem/self-confidence
- Prevent weight gain and obesity
- Prevent.manage lymphedema
- Prevent cancer cachexia
- Maintain independence
- Improved balance and strength
- Makes treatment more effective at destroying cancer cells
The benefits of exercise during recovery include:
- Increased range of motion
- Correct muscle imbalances that lead to pain and degeneration
- Increased energy
- Increased stamina
- Increases in strength and cardiovascular endurance
- Prevent osteoporosis, diabetes, lymphedema, future cancer, and damage to the heart and lungs
- Decrease body fat and increase lean muscle mass
- Improve balance and fall prevention
- Improved self-esteem/self-confidence
Based on the tremendous amount of evidence to support the aforementioned lists, it is mind-boggling that so few cancer patients are told to exercise. For those who are given the green light to exercise, the big problem is not knowing where to start, how to safely progress, and how to prevent many of the complications associated with cancer treatment.
By training more allied health professionals worldwide, CETI is creating a global resource for medical professionals to be able to confidently refer their patients.
“Cancer strips you of everything. Your hair, your body parts, your dignity, your self-confidence, your strength and stamina, your finances, sometimes even your job or spouse. A Cancer Exercise Specialist can help the cancer patient regain control of their life and their body at a time that the patient feels they have no control.” – Andrea Leonard
If you are interested in learning more about becoming a Cancer Exercise Specialist in Australia or New Zealand, or would like to learn about bringing CETI’s training to your country, please contact CETIguru@gmail.com
- Australian Institute of Health and Welfare 2019. Cancer in Australia: In brief 2019. Cancer series no. 122. Cat no. CAN 126. Canberra: AIHW.
- Australian Institute of Health and Welfare 2012. Cancer incidence projections: Australia, 2011 to 2020. Cancer series no. 66. Cat. No. CAN 62. Canberra: AIHW.
- Australian Institute of Health and Welfare & Australasian Association of Cancer Registries 2017. Cancer in Australia: in brief 2017. Cancer series no. 102. Cat no. CAN 101. Canberra: AIHW.
- Australian Institute of Health and Welfare & Cancer Australia 2008. Non-melanoma skin cancer: general practice consultations, hospitalisations and mortality. Cancer series no. 43. Cat. no. 39. Canberra: AIHW.
- Australian Institute of Health and Welfare 2018. ACIM (Australian Cancer Incidence and Mortality) Books. Canberra: AIHW
- Australian Institute of Health and Welfare 2013. Health system expenditure on cancer and other neoplasms in Australia: 2008–09. Cancer series no. 81. Cat. no. 78. Canberra: AIHW.
- Cancer Australia 2016. Cancer research in Australia 2016 to 2018: Opportunities for strategic research investment – Highlights, Cancer Australia, Surry Hills, NSW.In 2015, there were 131,452 new cases of cancer diagnosed in Australia (71,959 males and 59,493 females). In 2019, it is estimated that 144,713 new cases of cancer will be diagnosed in Australia (78,081 males and 66,632 females). In 2019, it is estimated that the risk of an individual being diagnosed with cancer by their 85th birthday will be 1 in 2 for both males and females.