
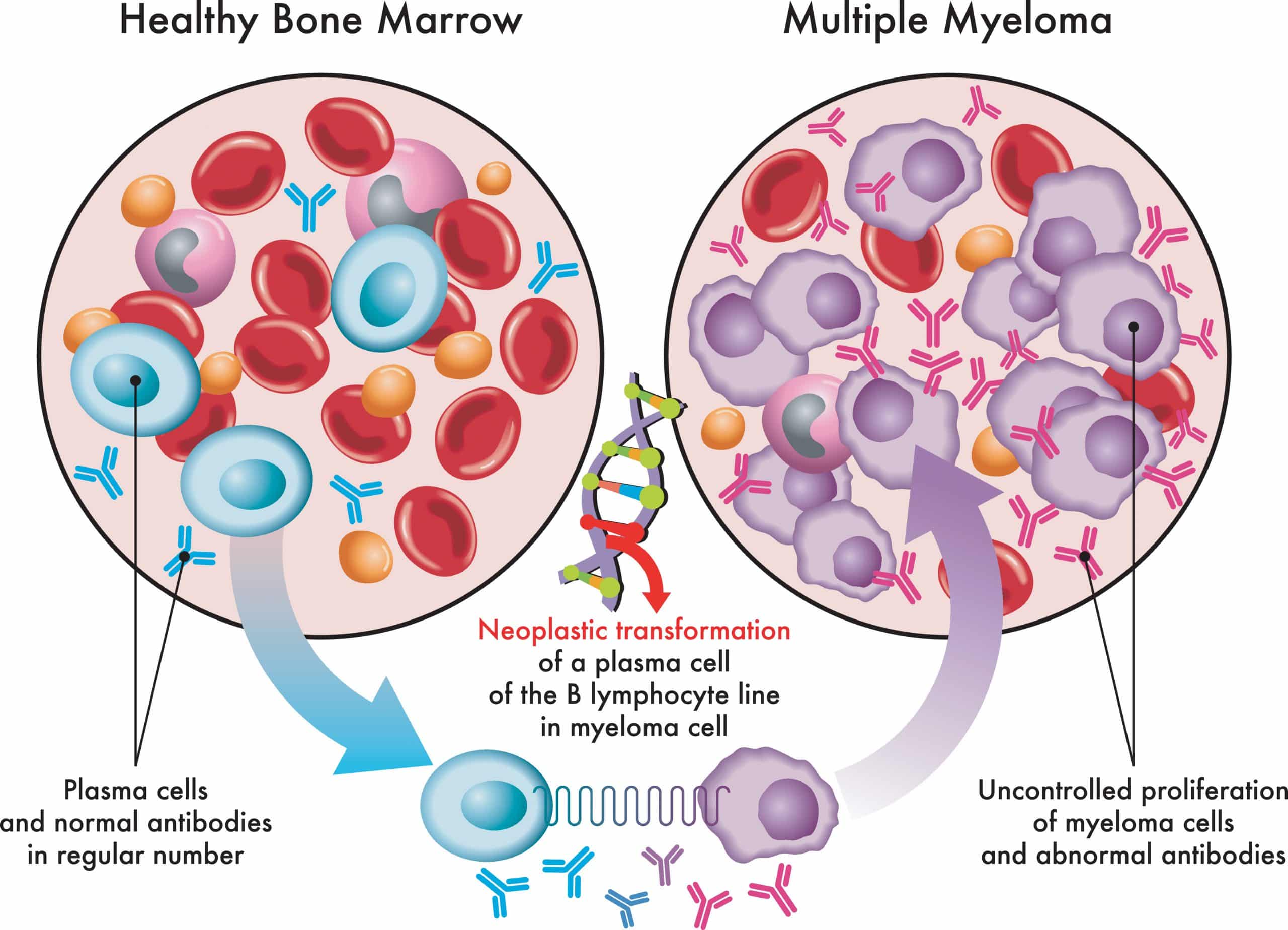
Customized Exercise Programming – Multiple Myeloma
 Tom received a referral for a client with stage III multiple myeloma (MM) and a life expectancy of 2-3 years. Tom has been a Cancer Exercise Specialist for two years, and this is his first client with MM. He asked if he could hire me to help her with Frank’s exercise program and teach him how to put the program together. He completed his initial assessment and health history and shared the following information with me:
Tom received a referral for a client with stage III multiple myeloma (MM) and a life expectancy of 2-3 years. Tom has been a Cancer Exercise Specialist for two years, and this is his first client with MM. He asked if he could hire me to help her with Frank’s exercise program and teach him how to put the program together. He completed his initial assessment and health history and shared the following information with me:
- Frank is 52 years old and was an avid exerciser prior to his cancer diagnosis.
- He is 6’2″ and currently 180 lbs. He has 17% body fat.
- He is currently on a combination of bortezomib, lenalidomide, and dexamethasone
- His blood counts show moderate leukopenia and thrombocytopenia
- He is currently undergoing chemotherapy and plasmapheresis
- He has painful neuropathy in both hands and feet and has a difficult time standing
- He has lyctic lesions and compression fractures in L4/L5
- He has trouble sleeping, and elevated blood sugar levels, due to the steroid medication
- He has extreme fatigue and chemo-brain
- He has a difficult time with her short-term memory and completing basic tasks
- His BP is 110/85 and her RHR is 78.
- Moderate upper-crossed syndrome
- Moderate anterior pelvic tilt
- Struggles with balance on both sides
- Avoid squat test because of compression fractures
- Modified Thomas Test confirms tight hip flexors and quads on both sides.Tom is overwhelmed with the combination of Frank’s treatment, side-effects, and physical assessment as well as his concern for spinal cord compression. He is not sure where to begin.
 I started by compiling my own notes and breaking everything down for him one step at a time.
I started by compiling my own notes and breaking everything down for him one step at a time.
- Because Frank has neuropathy in his hands, Tom will need to choose upper body exercises that don’t put him at risk for dropping the weights or letting go of the bands. He will focus on machines and isometrics for his upper-body workout. Because Frank also has neuropathy in his feet, he will avoid all high impact activities completely and start with a recumbent bike for cardio because of his elevated risk of falling, bruising easily due to low platelets, and discomfort and pain. When he is through with treatment and his blood counts are good, swimming will be a great option. Frank has trouble with balance because of the neuropathy and extreme fatigue so balance work will be critical.
- Since Frank began chemotherapy, he has been vomiting several times per week which has added to his fatigue.
- On days that Frank has vomiting, he will need to avoid exercise for 24-36 hours and make sure that he re-hydrates and replenishes electrolytes. If he has spells of nausea, Tom will tell him to stop exercising, sit down, and drink water. If the feeling does not pass, he will suggest that Frank go home.
- Tom will also incorporate lower-body ‘functional’ exercises, starting with wall-sits and working up to wall squats with a small physioball supporting lumbar area to help increase his bone density and perform activities of daily living. He will also work with Frank on gentle stretches for his adductor complex, quads, and hip flexors. Cardio will help to strengthen his heart and lungs, increase his energy, and help him lose body fat.
- Because of the upper-crossed syndrome Frank needs to stretch both his pecs and lats. He should focus on shoulder retraction and depression to stabilize his shoulder girdle. To strengthen the opposing upper/middle back muscles he will start with isometric reverse flys and shoulder scaption – just a few repetitions to begin with.
- Because Frank is extremely fatigued, Tom is suggesting he exercise for 20-30 min. 3-4 times a week, or as-tolerated. Since he is currently undergoing treatment (and extremely fatigued and low-functioning), he should only be at 20-40% of his Karvonen heart rate. Because of COVID and Frank’s already compromised immune system, Tom arranges ZOOM calls for their workouts. Frank always has someone there in his home during his exercise sessions to help with balance, prevent injuries, and be there in case of an emergency.
- Tom wants to get Frank in a swimming pool when his blood counts improve and COVID is not an issue.
- Tom will refer Frank to a Registered Dietician who specializes in oncology to help put together a meal plan that will ensure that he is getting the appropriate nutrition and help with building lean-muscle mass.
Once I gathered my thoughts, I was able to come up with the following workout routine for Tom to facilitate with Frank for his initial 6-8 weeks.
DAILY deep breathing exercises and 10-minutes of meditation and gratitude. Frank will use the recumbent bike in his living room for 5 minutes a day (when he has the energy), working up to 10-15 minutes each day as tolerated. If his energy is really low, he can break this into 5 minute increments (or whatever he can do without becoming more fatigued). Done properly, Frank should feel energized (or at least no more fatigued than when he started). Following his cardio session, Frank will do a corner or door stretch for his chest (careful to avoid an excessive pelvic tilt and stress on his lumbar spine), a lat stretch while sitting on a chair and sliding both arms forward on his kitchen table (palms facing one another), and a quad/hip flexor stretch while seated with one leg hanging off of the side of the chair (focusing on engaging glutes and avoiding excessive anterior tilting). Tom will also give Frank a routine to help minimize some of his neuropathy side-effects for upper body and lower body.
Balance exercises and core exercises will be critical for fall and injury prevention. Tom must make sure that Frank has something stable to hold on to or has a spotter in the house and nearby. Tom encourages Frank to sit on a 75″ physioball placed in a corner. His spotter should be standing in front of him so that he has little-to-no chance of falling. He will proceed with “pelvic clock” in each direction. Since the doctor has advised against lumbar flexion and extension, pelvic tilts should be avoided for the time being.
2 x PER WEEK Lower-body strength training – starting with functional training. Frank will place a band around his thighs and push his thighs outward during his wall-sit. The goal is 3-4 reps (holding each for 10 sec. or as long as Frank can tolerate) and stop if he gets too fatigued. Tom will also have Frank do side-lying clams. Frank will place a pillow under his head and make sure his spine is in alignment. They will aim for 8-10 reps on each side. Fatigue will be the determining factor for the number of reps as they progress. As it becomes easier, Tom may suggest that Frank add a circular band around his thighs to add resistance. Tom needs to make sure that whatever they do gives Frank more energy rather than causing him to be more fatigued.
On two of the non-leg days Frank will perform exercises that challenge his memory. Tom will have Frank perform a set of 6 reps of a particular movement; let’s say toe raises. Then he will add another exercise; maybe seated rows on a physioball. Frank will have to remember the first set of toe raises, perform 6 of them, do another set of rows, and then Tom will add another exercise and so on and so on. Frank may get frustrated when he can’t remember what comes next and Tom can remind him that many of the side-effects of treatment will lessen or go away completely over time. Tom will encourage him to keep pushing ahead, but also knows when Frank needs to take a “step back.”
Tom will re-assess Frank in 8-12 weeks and either continue with this routine, or progress to longer duration of cardio, more repetitions, and the addition of more strength training, multi-planar, and balance exercises.
**Keep in mind that the long-term risk of osteoporosis, diabetes, damage to the heart, lungs, and kidneys, and risk of future cancers is elevated due to chemotherapy and adjuvant medications. Therefore, a proper balance of strength training, cardio, and weight and stress management is critical for survivorship and quality of life.
**Because spinal cord compression is a concern with patients with MM you must be aware of any sudden changes in cognition, mobility, and reflexes and have them contact their doctor IMMEDIATELY if they are symptomatic. The sooner it is diagnosed, the better the long-term prognosis.
If you are in need of assistance with a special-needs or physically-challenged client, you can get Andrea Leonard’s help in with custom exercise programming.